WELCOME TO NAGAR PALIKA PARISHAD HASANPUR
swakar
सर्विस लेबल बेंच वर्ष 2018_19
सर्विस लेबल बेंच वर्ष 2019_20
वित्तीय वर्ष 15-16,16-17 एंव 17-18 का आडिट शीट/ बैलेंस शीट
बजट वित्तीय वर्ष 2017-18,2018-19,2019-20
Balance Sheet 2016-17,2017-18,2018-19
स्वकर वसूली कैंप
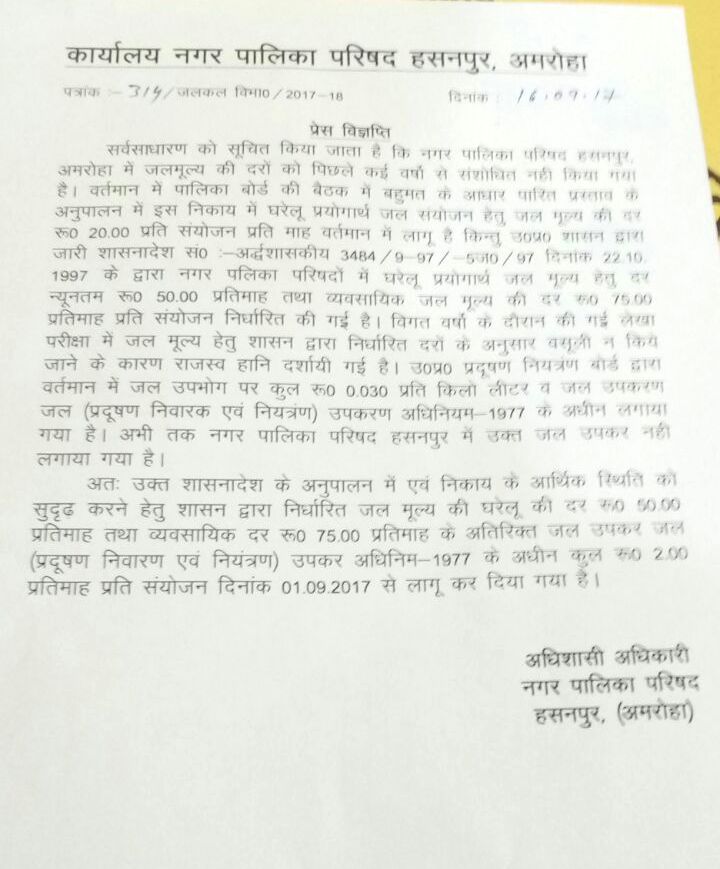
WaterCharge New Rates effectec from 1st Sep 2017
Grah kar me 5% ke discount ka laaf uthayen
बजट वित्तीय वर्ष 2014-15, 2015-16, 2016- 17, 2017- 18
वित्तीय वर्ष 14-15, 15-16 एंव 16-17 का आडिट शीट/ बैलेंस शीट
सर्विस लेबल बेंच वर्ष 2017- 18
{kind=link}
{kind=link}




